Planning applications for clinics rarely fail because the treatment rooms look the wrong colour. They run into trouble because movement, access and parking haven’t been thought through early enough. That is especially true for an Aesthetic, Wellness And Beauty Clinics In High Streets Or Mixed-Use Locations Transport Assessment, where local planning and highway officers will want clear evidence on trips, servicing, kerbside pressure and accessibility.
In 2026, this is no longer a niche issue. High streets are being reshaped around active travel, bus priority, short-stay turnover and mixed-use regeneration. At the same time, aesthetic, wellness and beauty operators are taking units in town centres, upper floors, parade frontages and mixed-use blocks because that is where demand is visible and rents can still work. The planning case may look straightforward on paper, but transport effects can be more nuanced than many applicants expect.
We approach these assessments as practical planning tools, not box-ticking exercises. For architects, planners, surveyors, lawyers, developers and local authorities, the real question is simple: will the proposed clinic function safely and efficiently within its street and policy context? The answer usually depends on how well the assessment explains likely trip patterns, parking demand, servicing, disabled access and sustainable travel opportunities. Done properly, it reduces uncertainty and keeps applications moving. Done badly, it invites requests for more information, objections and avoidable delay.
Key Takeaways
- A clear transport assessment for aesthetic, wellness and beauty clinics in high streets or mixed-use locations ensures safe, efficient operation and strengthens planning applications.
- Appointment-led clinics benefit from staggered bookings to manage trip patterns and reduce kerbside congestion.
- Local authorities prioritise evidence on trip generation, parking demand, servicing, disabled access and sustainable travel over general assumptions.
- Drop-off management and short-stay parking are critical in dense urban settings to prevent disruption on constrained kerbside spaces.
- Tailoring transport assessments to local policy and site specifics reduces delays and avoids requests for further information.
- Early engagement with planning and highway officers helps align transport assessments with local expectations and policies.
Why Transport Assessment Matters For Clinic Planning Applications
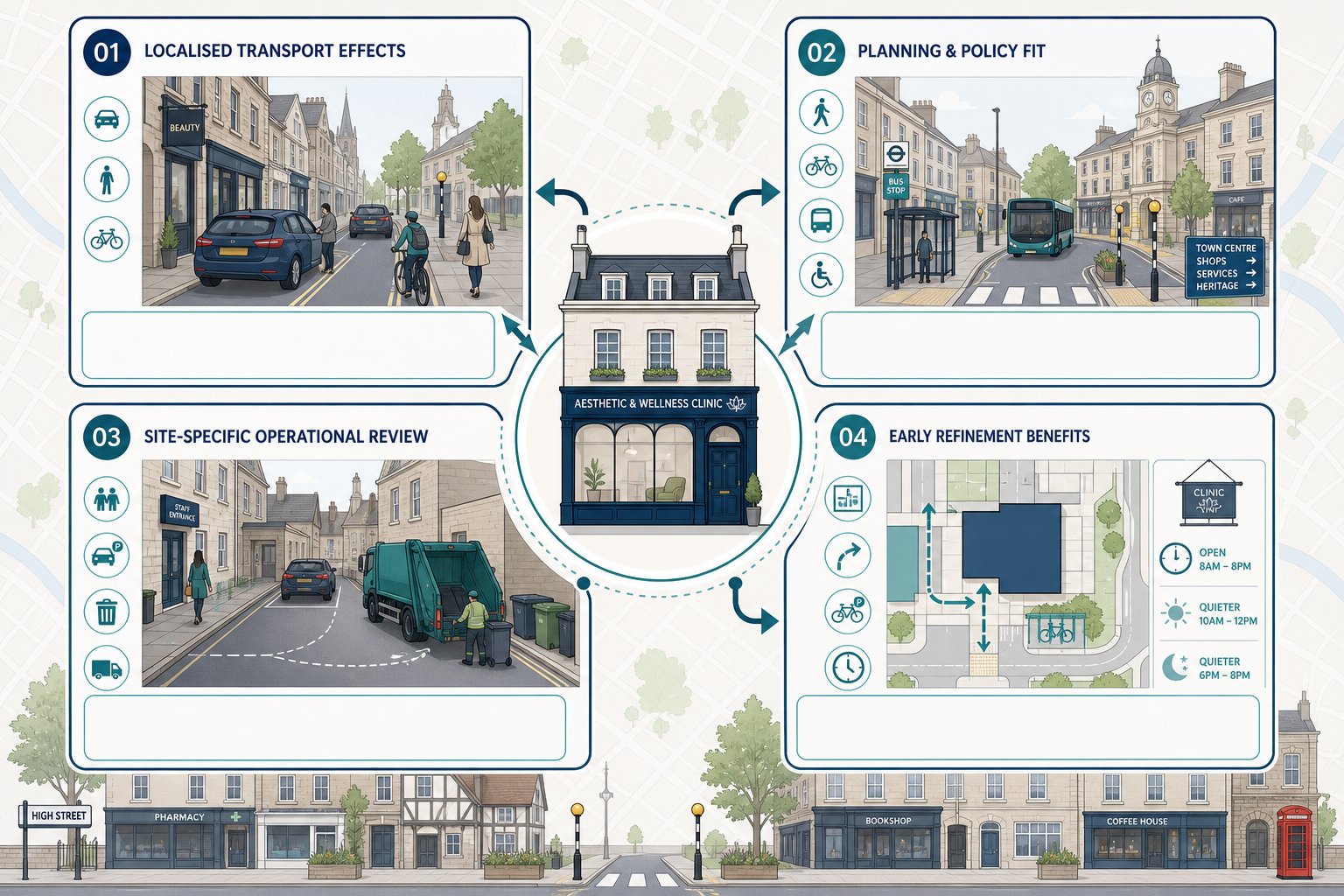
A transport assessment matters because clinic uses can appear low impact at first glance while still creating quite specific localised effects. Aesthetic, wellness and beauty clinics tend to sit in sensitive urban environments: high streets with constrained kerbsides, mixed-use corridors with competing demands, conservation areas, and centres where councils are trying to rebalance street space away from general traffic. In that context, even modest schemes need a clear explanation of how people will arrive, where short-stay activity will sit, and whether highway safety will be protected.
For planning teams, the assessment does three jobs at once. First, it tests whether the use would create unacceptable effects on network operation, access or parking. Second, it demonstrates policy compliance, particularly around active travel, accessibility and town-centre-first thinking. Third, it gives officers confidence that the applicant understands the site rather than relying on generic assumptions.
That last point is often what separates a smooth determination from a prolonged one. A clinic may have fewer trips than a restaurant or gym, but if the proposal ignores drop-off patterns, staff parking restraint or waste collection arrangements, highways comments can quickly become detailed. Our experience is that concise, tailored reporting usually works better than overblown theory. A focused transport assessment for the actual planning questions can head off requests for further information before they arise.
And importantly, a good assessment does not just defend a proposal. It can also refine it early, while changes to layout, hours, servicing or cycle provision are still easy to make.
How High Street And Mixed-Use Settings Change The Transport Picture
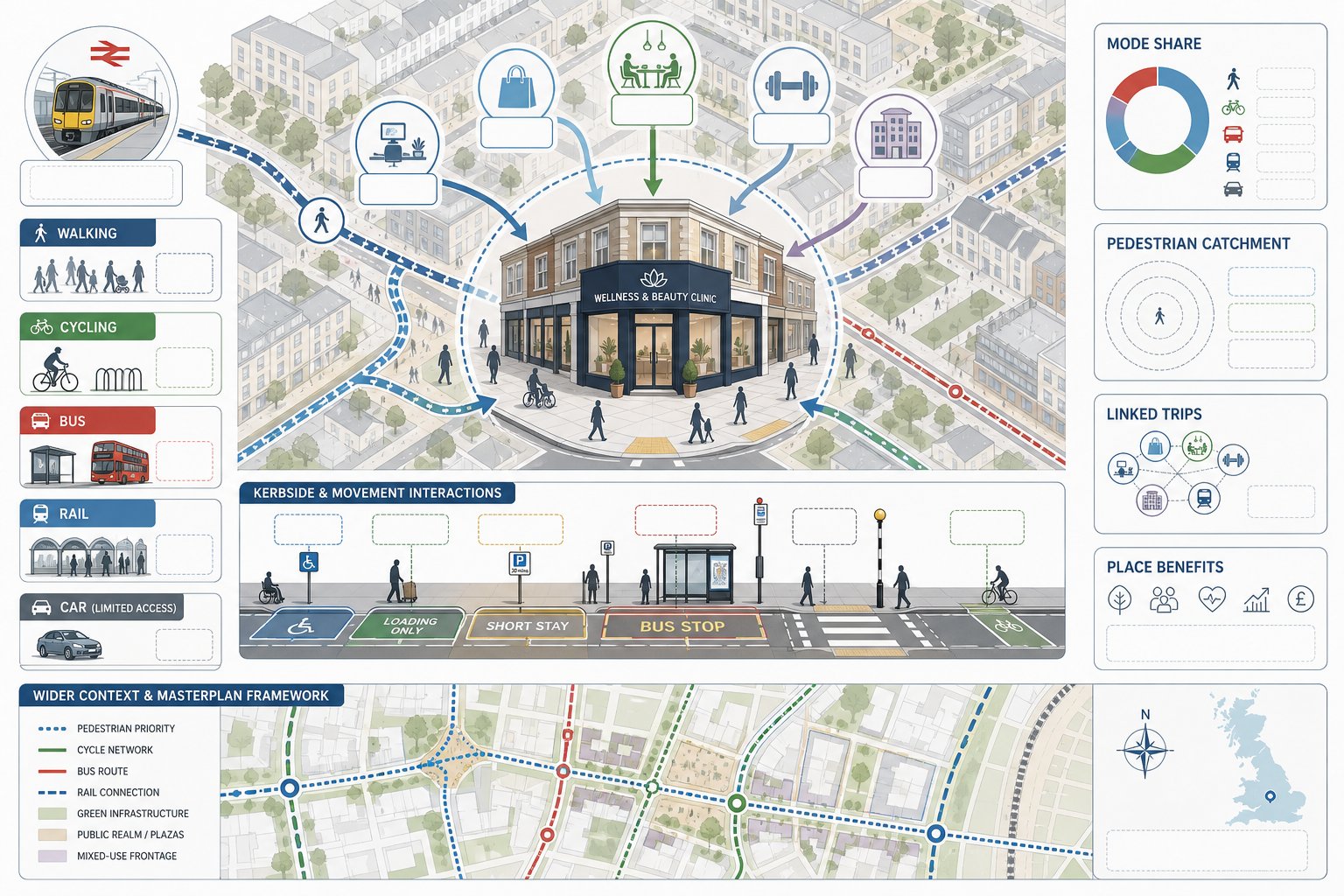
High street and mixed-use locations are not transport “standard cases”. They usually have stronger public transport access, denser walking catchments and more linked trips than edge-of-centre or out-of-centre premises. That can work in the applicant’s favour, but only if the evidence reflects it properly.
On a typical high street, parking is limited, turnover matters, and informal stopping can be more contentious than overall traffic generation. A clinic that relies on pre-booked appointments may generate modest net new demand, yet a handful of poorly managed pick-ups or deliveries can cause disproportionate concern. Councils know this. So they often focus less on gross trip numbers and more on kerbside behaviour, disabled access and compatibility with nearby loading, bus stops, crossings and cycle lanes.
Mixed-use settings introduce another layer. Trips are often shared with retail, work, food and leisure activity, so not every clinic visit is a single-purpose car journey. Someone may walk from an office, combine a treatment with shopping, or arrive by rail and continue on foot. In strategic terms, that often supports a lower car mode share than suburban comparators would suggest. But those assumptions still need evidence.
This is where site context becomes central. Schemes in regenerated centres or larger blocks benefit from being read alongside wider movement strategies, particularly where a mixed use masterplan already establishes access, parking management and pedestrian connections. We usually find that the strongest assessments explain not just how the clinic generates trips, but how the surrounding place absorbs them.
Typical Trip Patterns For Aesthetic, Wellness And Beauty Clinics
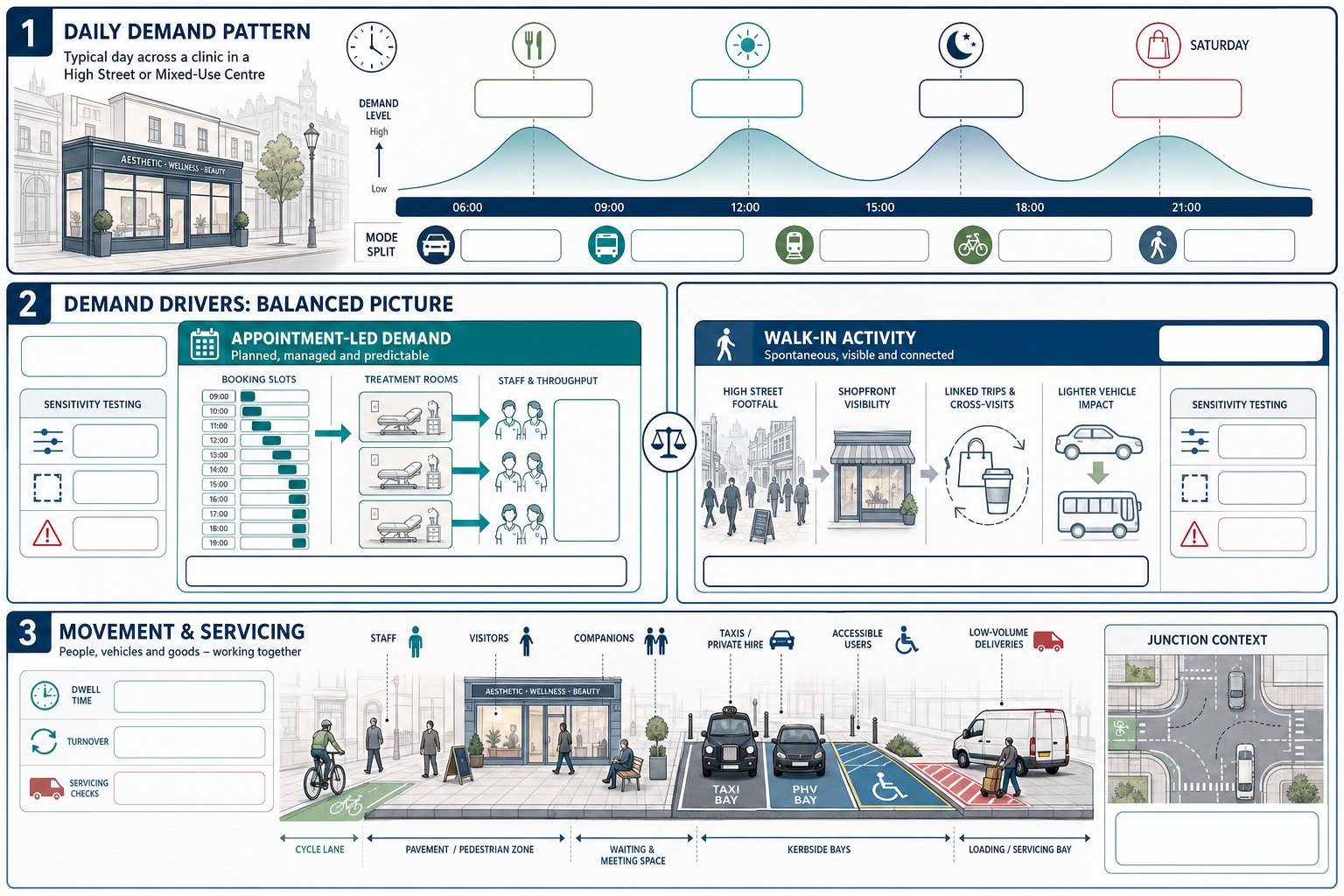
Trip patterns for these clinics are usually distinct from mainstream retail and quite different from primary healthcare. Demand is often spread through the day, with pulses around lunch, late afternoon, evening and Saturdays. The busiest periods are not always the highway network peaks, which can be helpful, but overlap still matters where staff arrivals coincide with commuter activity or where after-work bookings add pressure to short-stay bays.
Catchments are commonly local to sub-regional. Smaller beauty and wellness operators may rely heavily on nearby residents, workers and pass-by trade. Higher-value aesthetic clinics can draw from a wider area, particularly where specialist treatments are offered. That means one category label is rarely enough. The likely client profile, treatment length, pricing and brand position all influence travel behaviour.
Another recurring point is dwell time. A 15-minute appointment, a 45-minute treatment and a two-hour procedure do not produce the same parking turnover profile, even if daily trip totals look similar. Likewise, upper-floor clinics with controlled reception access often behave differently from active ground-floor units.
For that reason, we avoid defaulting to broad assumptions. Comparable trip rates, local surveys, booking patterns and site-specific judgement are usually needed to explain demand credibly. Where proposals sit within larger planning contexts, methods used on other sectors can also be instructive: the discipline behind a Residential Development Transport study, for example, often translates well in terms of mode share, parking stress and accessibility analysis.
Appointment-Led Demand Versus Walk-In Activity
Appointment-led demand is generally easier to assess because the operator can cap throughput. We can estimate the number of clients per hour, match that to staff levels and treatment room capacity, and build a realistic picture of arrivals and departures. This tends to support a more stable trip profile with fewer sharp surges, especially where bookings are staggered. It also helps when discussing mitigation, because management measures such as slot spacing, text reminders or staff travel plans can be linked directly to observed demand.
Walk-in activity is less predictable, but in high street locations it is not necessarily more harmful. Many walk-in customers are already in the centre for another reason. They may be passing the frontage, combining the visit with shopping, or arriving from nearby workplaces on foot. In transport terms, those linked trips can reduce net new vehicle demand.
The key is not to assume one model or the other without evidence. Councils often ask whether an initially appointment-led clinic could evolve into a more retail-like operation with greater impulse demand. If that risk exists, the assessment should address it openly through sensitivity testing, conditions on floorspace use, or operational descriptions that clearly define how the clinic will function.
Staff, Visitor And Servicing Movements
Staff movements often deserve more attention than applicants expect. In accessible centres, many staff may arrive by bus, rail, cycle or on foot, particularly where parking is expensive or unavailable. But not all clinics are the same. Early starts, late finishes, security concerns and the need to carry equipment can affect mode choice. We hence look at roster patterns, likely staff numbers by shift and whether arrival times overlap with local highway peaks.
Visitor movements include clients, companions and occasional clinical or maintenance visits. Companions are easy to miss in a transport note, yet they can influence waiting space, kerbside dwell times and short-stay demand. The same goes for accessible transport users, including taxis and private hire vehicles.
Servicing volumes are usually low compared with food, retail or healthcare uses. Even so, deliveries, laundry, consumables, waste uplift and occasional equipment replacement still need a lawful and practical arrangement. If vans are likely to stop on-street, the assessment should test whether that can happen without obstructing traffic, cycle lanes or pedestrian movement. On more sensitive sites, tracking software and junction testing may be useful: where vehicle interaction is material, Junctions 11 Software or swept-path work can provide the clarity officers need.
When A Transport Assessment, Transport Statement Or Technical Note May Be Needed
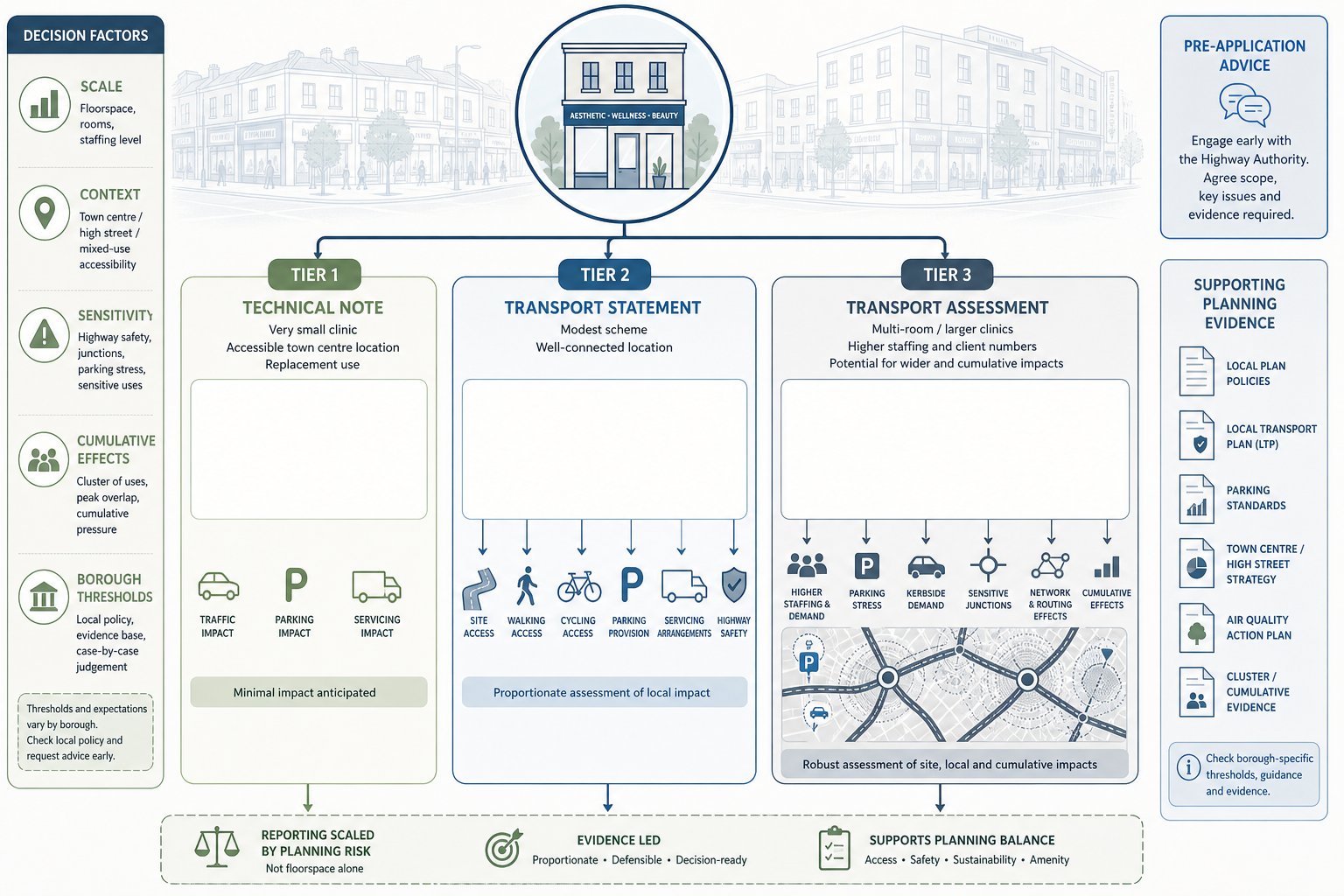
The right level of transport reporting depends on scale, context and sensitivity, not just floorspace. That is why two clinics of similar size can require different submissions in different boroughs.
A Technical Note may be enough where a very small clinic is proposed in an accessible centre, especially if it replaces another active town-centre use with similar or lower trip generation. In those cases, the planning issue may simply be to confirm no material intensification in traffic, parking or servicing. A short, focused note can often do that well.
A Transport Statement is more common for modest schemes: a new unit in a well-connected area, an upper-floor conversion, or a small expansion where effects are expected to be limited but still need structured evidence. Here, we would normally cover site accessibility, trip generation, parking, servicing, cycle parking and highway safety in enough detail to answer foreseeable objections.
A full Transport Assessment is usually justified for larger multi-room clinics, proposals with significant staffing, locations with known parking stress, or streets where kerbside demand is already contentious. It may also be required where the site sits within a wider redevelopment, close to sensitive junctions, or where cumulative effects need testing.
Pre-application advice is often worth the time. Thresholds vary by authority, and local validation lists can be surprisingly specific. Where broader development effects are part of the picture, the transport submission may need to sit consistently alongside an environmental impact assessment or related planning evidence. In short: match the report to the real planning risk, not just the label.
Key Planning And Highway Issues Local Authorities Often Examine

Local authorities usually examine clinic proposals through a practical lens: can the use operate safely and without causing unacceptable friction on the street? In 2026, that question is increasingly filtered through policy on healthy streets, town-centre vitality, accessibility and carbon reduction.
Parking standards are still relevant, but many councils no longer treat them as the whole story. They also look closely at likely mode share, nearby public car parks, staff parking restraint, cycle provision, and whether a proposal would increase informal stopping on yellow lines, in bus stop clearways or across crossings. Highway safety concerns can arise from very ordinary details: a difficult doorway threshold, poor visibility at a rear access, or deliveries that would reverse over a busy footway.
Authorities may also ask whether the use is genuinely akin to a clinic, whether it behaves more like personal services retail, or whether treatment intensity changes the likely trip profile. This matters because classification can influence trip assumptions and parking expectations.
Where the proposal forms part of a larger mixed-use or town-centre change, officers may consider cumulative effects as well. We often find that robust transport planning for one use benefits from consistency with wider development evidence and local strategy, much as it would in a broader transport assessment for developments: the methodology and framing should answer the authority’s actual concern, not simply repeat national guidance.
Access, Drop-Off, Parking And Loading Constraints
This is where many clinic applications either reassure officers quickly or trigger detailed follow-up questions. A premises can have modest traffic generation overall yet still fail if day-to-day access is awkward. We look first at the obvious basics: direct pedestrian access from the footway, level changes, door swing conflicts, visibility, and whether arrivals would spill into carriageway space or cycle tracks.
Drop-off is often a bigger issue than long-stay parking. Aesthetic and wellness clients may use taxis or private hire vehicles, and some may need to be collected after treatment. If there is no lawful place for short dwell times, the kerbside can become messy fast. Authorities hence want to know where vehicles will stop, for how long, and what happens when bays are occupied.
Parking analysis should distinguish between clients and staff. Staff parking can often be managed through permit restrictions, contracts, travel plans or use of public car parks. Client parking needs a more nuanced view of duration, turnover and nearby supply. Blue Badge provision, whether on-site or nearby, should be addressed explicitly rather than folded into general parking text.
Loading is usually lower key but still important. Timed deliveries, use of existing loading bays, or consolidated servicing through a landlord can all help, provided they are realistic and enforceable.
Walking, Cycling And Public Transport Accessibility
Accessible locations can be a major strength for clinic schemes, but only if the assessment proves accessibility rather than just claiming it. We normally start with the pedestrian environment: footway width, crossings, gradients, lighting, surveillance and step-free access from likely arrival points. Personal security matters too, particularly for evening appointments.
Cycling is often underplayed. In many centres, short urban trips to beauty and wellness appointments are well suited to cycling if routes are coherent and parking is secure. Officers may hence expect details of nearby cycle links, the quality of local infrastructure, and whether cycle parking is covered, visible and convenient. Staff facilities can also matter in larger units.
Public transport should be described in practical terms, not just distance circles on a plan. Which bus routes serve the site? How frequent are they at opening and closing times? Is the rail station realistically walkable for most users? In London, PTAL can be useful: elsewhere, comparable accessibility indices or timetable-based analysis may be more appropriate.
A short accessibility narrative grounded in actual conditions often carries more weight than pages of generic mapping. The goal is to show that sustainable modes are not theoretical options but realistic choices for staff and clients.
Evidence Commonly Used To Support A Robust Assessment
A robust assessment usually blends policy, observation and proportionate technical evidence. Policy comes first because it frames what the authority is trying to protect or promote. That normally means the National Planning Policy Framework, the local plan, parking standards, design guidance and any healthy streets or town centre strategies. Referencing policy is not enough on its own, though: the evidence must show how the proposal performs against it.
Trip generation evidence is often the most debated element. Comparable survey data, whether from TRICS-type sources or local surveys, can be useful, but clinic categories are not always perfect fits. We hence prefer triangulation: benchmark data, site observations, operator information, treatment room capacity and booking assumptions. Nearby land uses matter as context too, especially where linked trips are likely.
Mode share evidence may come from Census journey-to-work data, local travel surveys, centre studies or bespoke counts. Parking surveys can be critical in controlled parking zones or streets with known evening stress. Servicing evidence may include delivery schedules, waste collection arrangements and swept-path checks where manoeuvring space is tight.
For larger or sensitive schemes, capacity analysis may be needed, although many clinic proposals do not warrant heavy modelling. When they do, the method should be tightly scoped. It is usually better to answer one junction concern well than to produce a sprawling appendix no one trusts. The common thread is simple: use enough evidence to resolve the planning issue, and no less.
Common Risks That Delay Decisions Or Trigger Objections
The most common risk is underestimating how visible small transport problems become on a busy street. A proposal may generate only a handful of extra vehicle movements, but if those movements block a bus lane, occupy disabled space informally or force loading from the live carriageway, objections can come quickly.
Parking is the classic example. Applicants sometimes assume that because a site is central, parking barely matters. Officers may take the opposite view: central locations often have the least spare kerbside capacity and the strongest enforcement concerns. If client dwell times are longer than assumed, or if staff parking is left unmanaged, the authority will notice.
Another regular issue is weak treatment of servicing and drop-off. A sentence saying deliveries will be “minimal” rarely satisfies anyone. Highway officers want to know who delivers, when, in what vehicle type, and where stopping will occur. The same goes for taxis, private hire vehicles and accessible pick-up arrangements.
Disabled access and active travel are also frequent fault lines. If step-free routes, Blue Badge access, crossing quality or cycle parking are poorly addressed, the assessment can look dated very quickly. And finally, there is the procedural risk: failing to engage with early highways comments. Many delays happen not because the scheme is unacceptable, but because the applicant responds slowly or with generic addenda instead of targeted analysis. A crisp, evidence-led reply often saves weeks.
Conclusion
For clinic proposals in town centres, parade frontages and mixed-use schemes, transport is rarely the loudest planning issue at the start. But it is often the issue that determines whether an application moves smoothly or stalls. The strongest submissions are the ones that stay specific: they explain likely trip patterns, test kerbside realities, address disabled and sustainable access properly, and match the level of evidence to the scale of the scheme.
In our view, an effective Aesthetic, Wellness And Beauty Clinics In High Streets Or Mixed-Use Locations Transport Assessment is not about producing the thickest report. It is about answering the right questions early, in the language local authorities and highway officers actually use. When that happens, planning teams are in a far better position to secure timely decisions, proportionate conditions and workable outcomes on the ground.
Frequently Asked Questions about Transport Assessments for Aesthetic, Wellness and Beauty Clinics
Why is a transport assessment important for aesthetic, wellness and beauty clinic planning applications?
A transport assessment is crucial because it demonstrates that the clinic will not negatively affect highway safety, network capacity, or parking, while showing compliance with active travel and healthy streets policies. It reduces risks of application refusal or delays due to planning obligations.
How do high street and mixed-use locations impact transport considerations for clinics?
High street or mixed-use locations usually have strong public transport, dense walking and cycling options, and limited parking. Clinics here benefit from linked trips with retail or offices, which often reduces car use but require evidence reflecting this context for planning approval.
What are typical trip patterns for aesthetic, wellness and beauty clinics in town centres?
Clinic demand typically peaks during daytime, evenings, and Saturdays, with a local or sub-regional catchment. Trips combine public transport, walking, cycling, and car use, influenced by appointment lengths, treatment type, and clinic location, which must be reflected in transport assessments.
When is a full Transport Assessment needed versus a Transport Statement or Technical Note for clinic proposals?
A full Transport Assessment is usually needed for larger, multi-room clinics, sites with parking stress or sensitive locations. Smaller clinics or modest expansions in accessible centres may only require a Transport Statement or a brief Technical Note verifying no material traffic intensification.
How should parking, drop-off and servicing be addressed in transport assessments for these clinics?
Assessments must show safe pedestrian access, Blue Badge provision, managed staff parking, and clear plans for short-stay drop-off including taxis and private hire vehicles. Timed servicing and designated loading bays should prevent obstruction of traffic and cycle lanes.
What key evidence supports a robust transport assessment for clinics in urban settings?
Robust assessments combine local policy references, trip generation data from sources like TRICS, mode share statistics, parking and servicing surveys, and may use tools like Junctions 11 Software for capacity analysis to effectively address planning concerns.